
A trend is growing within the alternative medicine industry that should be addressed by our rantiness.
This new boss looks alot like the old boss, just dressed in modern trappings of technology, with its misinformation circulated by modern propaganda machines. At its core, it’s nothing more than it’s ever been… snake oil.
“Practitioners” are promoting genetic testing for a relatively common enzyme abnormality. They link this to a host of diseases; all the things wrong with your life can be connected to this gene, it seems.
Spearheading this is a fake doctor lacking any credentials relevant to the discussion. And guess what? If you have said problem, special supplements can fix it!
There’s a chance some of this discussion may be new to you. You may be unfamiliar with the claims alternative practitioners are making, the diagnostics they are bending to their narrative, or the “treatment” regimens thrown at patients, whom I believe are victims in all of this. We’ll try not to bore you.
Today we discuss MTHFR abnormalities and the B-Vitamin Bonanza plaguing the alternative medicine world.
The MTHFR Doomsday Talk
I want to take a moment to set the stage a bit. There is a naturopathic doctor, Ben Lynch, who is leading a herd of “practitioners” down a road of misinformation.
As a result, their patients are paying for unnecessary testing and taking high doses of unnecessary supplements. The promise they make is a reduction in all things horrible – heart disease, cancer, Alzheimer’s – all the Boogeymen whom we fear.
They use accessible genetic tests to identify victims/targets/patients. Someone who reads their propaganda takes the plunge, and subsequently finds their own testing puts them in this “high-risk group” would obviously be fearful and motivated to action.
Thankfully for the quacks, this means spending money on supplements they sell.
As a reminder to new readers: I sell supplements. It’s in my interest to sell more. Unlike a majority of others in the same business, I feel like I’d rather do the right thing – only recommending what people really need while offering clean, potent, pure versions of anything they could want.
We sell stuff, but I’ll only recommend something that at least has some decent science to it.
And this stuff Lynch promotes reeks of bad science. In fact, it’s the polar opposite of good science.
Who is Ben Lynch, really? Can we trust him? SPOILER: NO! What is MTHFR and how does it all relate? It isn’t just how you could abbreviate a bad word (read the abbreviation again – you’ll get it if you have a low brow sense of humor like me…).
All these questions will be answered, don’t you worry!
WTF is the MTHFR?
MTHFR is an important enzyme called methylenetetrahydrofolate reductase. It isn’t the world-ending lynchpin these quacks make it, though. I’m going to try to keep this all as simple as I can. Let’s use pictures.
Remember our talk about proteins, where we said there are essential and non-essential amino acids?
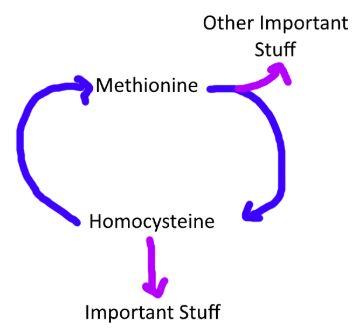
Essential amino acids are those we can’t make and need to get from our diets. One, methionine, is important because it creates a non-essential amino acid called homocysteine.
There’s a magical loopty loop where methionine is used to help make homocysteine. Since our body is very efficient, it recycles extra homocysteine back to methionine.This is important! Around and around:
The process of making and using homocysteine is relatively complicated, involving amino acids, enzymes, and B vitamins (B6, B12, and even B9 – folic acid) to name a few of the players. In the alternative medicine world, people call this process “methylation”, but that’s dumb.
It’s dumb because methylation is a chemical process where anything donates a methyl group, not this specific pathway or process. But many will substitute “methylation” for this process. A more apt name is the “methyl cycle.” Anyway…
One of the enzymes, MTHFR, converts folic acid and dietary folate into a compound that makes this process possible.
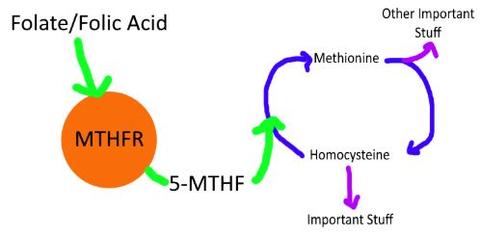
If we can’t make 5-MTHF, we can’t turn homocysteine back into methionine, and homocysteine builds up in the blood.
Again, this “methyl cycle” is complicated. There isn’t one fault-point where everything implodes. There would have to be lots of backup in multiple points for homocysteine to get too high. Typically it’s because of a deficiency in B-Vitamins, among other things.
Homocysteine is a troublemaker. If homocysteine levels elevate, it can do some damage. Homocysteine can damage DNA and even blood vessels. It can lead to thickening and clogging of the arteries, leading to stroke or heart attack. Serious stuff.
We also know that micro and macrovascular (small and large blood vessel) disease contributes greatly to Alzheimer’s risk. High homocysteine levels are present in someone with cardiovascular disease AND people with a high risk for cardiovascular disease.
So while homocysteine levels can be elevated in people with Alzheimer’s, and if you have high homocysteine you are at a higher risk of developing Alzheimer’s, we, the scientific community, don’t think homocysteine ALONE is the reason you have these higher risks.
There is a correlation, not causation. I’ll demonstrate my point with my favorite graph:
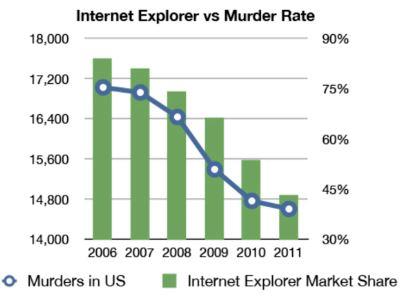
As the graph shows, as the number of people using Internet Explorer decreased, so did the murder rate.
They are somehow related (their numbers both go down), but it is pretty obvious one does not cause the other.
High homocysteine levels during pregnancy will lead to neural tube defects, pre-eclampsia, and all sorts of fun for the mom-to-be. We know this and are extremely familiar with the prevention of these problems.
Folic acid is a mainstay before and during pregnancy nutritional management. Most of our foods are fortified with folic acid to prevent this. There is no direct connection between folic acid, homocysteine, and miscarriage.
Homocysteine levels elevate when you have too few B-Vitamins, specifically B6, B9 (folic acid), and B12. Homocysteine can also be elevated in patients with chronic alcohol consumption.
Finally, genetic abnormalities in MTHFR can cause homocysteine to elevate. Basically, the homocysteine factory backs up and homocysteine rises.
As you can see, I’ve set you up. I’ve told you homocysteine can be harmful. Alzheimer’s! Heart disease! I’ve told you the causes of it, one of them being something you can’t control. What would you want to know, right now? “Do I have the genetic abnormality?!?!?” I’ve got just the thing for you…
Genetic Testing, Delivered
With advances in our understanding of the human genome along with the thrill of getting our consumer goods in the mail, many companies have popped up offering DNA testing, delivered right to your door.
Don’t go to that pesky doctor, with all his science, then to the lab with all their training… Just swab and send us, a private, for-profit company, the literal programming to what makes you, you.
Many people are curious about their genetic makeup. “I’m 10% Asian, but I’m a white guy… Genghis Khan you rascal!” Some people want to know if they are genetically predisposed to diseases because they don’t have enough to worry about in 2018.
These companies promise to tell you both. The funny thing is, they don’t interpret the results – they just give you the data. You have to feed your results into another app to appropriately “read” them.
And guess what they’ve found? Over 40% of us, approximately, have genetic mutations on the MTHFR gene! GASP!
Let’s do a mini rant here. Lightning round style:
- They aren’t telling you anything about your heritage. They’re just comparing you to those “purebreds” from specific areas. What they really say is if you share genes with some guy or gal whose family never left Ireland, for example. You’re not literally 34% Irish, you just share genes with people who are from there.
- How shady is it that they don’t even interpret their own results? You know why? Because they aren’t recognized as legitimate tests.
- Most importantly: privacy. Companies can’t keep your name, date of birth, social security number, or credit card info safe. You want to give them your DNA?
Just as I’ve told you to never use a pyramid scheme, I mean, MLM, I’d advise you to not bother with at home genetic testing. Besides the three reasons above, the big one is the simplest: Just because you have a genetic mutation, that doesn’t mean you’ll have a disease.
Your body is resilient and finds a way around little hiccups. A genetic marker that is abnormal isn’t a death sentence. Our fate is not sealed. Especially when it comes to this MTHFR.
MTHFR Genetic Testing – The Truth
So you’ve decided you want to do the genetic testing anyway, just like all those people who bought thousands in LuLaRue leggings hoping to turn a nice profit working from home… (That company is collapsing as we speak)
The results are in! Oh no, you DO have the MTHFR mutation! Does this mean you have to take action now or die of Alzheimer’s tomorrow like your quack/”practitioner” is telling you? No. It doesn’t. In fact, it means very little.
Here’s the truth. Many of us (again, over 40%!) have some sort of abnormality in the expression of the gene that programs your MTHFR enzyme.
The MTHFR doesn’t have an on and off switch; there are varying degrees of activity of MTHFR, so having an abnormality is meaningless.
MTHFR will work all the way down to as low as 20%. “But couldn’t I have less than 20% functionality?” No – if you don’t know it, you don’t.
Literally, almost all of us will retain MOST function of the MTHFR despite genetic abnormalities. Some will not, of course. It is rare… like 50 cases worldwide rare.
Those people have developmental disorders and seizure disorders and all sorts of horrible things. But they also can STILL have up to 20% function remaining in their MTHFR.
So if you haven’t spent much of your time in a hospital already dealing with this problem, it’s not a problem.
The MTHFR is just one part of a complex cycle turning methionine into homocysteine. There are other pathways to maintain proper homocysteine levels. Someone would have to have SEVERE (50 out of 7 billion) MTHFR abnormalities to have a clinical issue.
It does not matter that you have some genetic abnormalities of your MTHFR. All that matters is the end result: do you have high homocysteine levels and low folate and other signs of anemia?
If your homocysteine levels are high, we COULD be concerned that the orange thing isn’t making 5-MTHF:
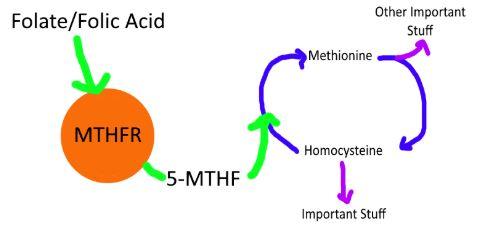
All we care about is getting 5-MTHF, right? It doesn’t mean we need a gimmicky test to definitively know if we are one of the rare people whose orange circle isn’t working right. You just need some extra 5-MTHF.
You know what 5-MTHF looks like? It looks like this:

Live-action shot as I type! (Who’s holding the camera??)
5-MTHF is l-methylfolate, the form of folic acid we recommend everyone use no matter what. It’s the active form. We don’t need no stinking orange circle!
The Cleveland Clinic and Mayo Clinic – both organizations that make money on billing for tests – have stated there is no reason to test for MTHFR abnormalities.
Most importantly, the national testing organization, the American College of Medical Genetics and Genomics, have said there is no evidence supporting testing the MTFHR genes. Download the full statement here.
So before the “Big Pharma wants to take our guns!” crowd comes in, let’s remember some stuff here. Big Pharma and the medical industry makes money on tests. They want to increase costs!
There are two companies who make 5-MTHF, which is THE “treatment” for MTHFR problems: Gnosis and…. MERCK.
Literally, Big Pharma makes the cure found in not only the prescription forms but in the supplements most people use. (Our supplier is Gnosis) Big Pharma is connected to the supplement industry and WANT you to believe they aren’t.
Genetic testing for MTHFR abnormalities is expensive, unnecessary, and meaningless.
Ask the RIGHT Question About MTHFR
Ben Lynch and his ilk have reframed a common medical situation and restructured it to fit their narrative. They start at the ABSOLUTE end of one incredibly rare pathway of a diagnosis algorithm and have convinced us that we ALL need to work backward from there.
But the right question to ask is the same as the question has ever been: What’s going on with my homocysteine levels?
Hopefully your answer is, “I don’t know.”
If homocysteine is an associate of the Boogeymen (heart disease, Alzheimer’s), we’d want to know where he is at all times. It’s not something we look for unless we have reason to, though, since most of us will have normal homocysteine levels. Here’s when we’d take a look:
- If we have signs of anemia on a Complete Blood Count, your doctor may order a Folate and B12 level. If these are abnormal, your doc may order a homocysteine level.
- If you have unhealthy cholesterol levels
- If you have had a heart attack or stroke
Most of us won’t really care what our homocysteine level is because we don’t have any issues that would cause it to be high.
If you’re in the camp that you’d like to know if you have the MTHFR and were about to blow hundreds on that test, take pause. At your annual physical, ask your doctor for a folic acid, B12, and homocysteine level.
They may oblige, and then you’ll know. If they don’t, don’t presume it’s because they’re a bad doctor. Instead, realize that they don’t want to run wasteful tests, which is what we all SHOULD want.
Let’s Talk About MTHFR Quacks
Many medical professionals – physicians, experts in genetics, experts in cardiovascular disease, experts in Alzheimer’s – have weighed in on Mr. Lynch’s approach and have unanimously called out the B.S.
Mr. Lynch isn’t a real doctor. He hasn’t gone to medical school. He isn’t an MD. He got a Naturopathic Doctor degree in 2007, which is comprehensive for alternative medicine, but it’s just a sliver of a fraction of what training a physician must undergo.
Mini Rant 2 for this month: In my opinion, we need to have some clear-cut, nationwide standards set so consumers aren’t confused about what training someone has and what their credentials are.
In New York, for example, the words “drug store” and “apothecary” are protected words. Meaning, if you call your sandwich shop the “Bagel Apothecary”, you’re in violation of state law and will be at best asked to rename and at worst fined.
I feel this should go the same for doctors. I feel like those rules and definitions should be as uniform as humanly possible from state-to-state. /end min rant
So Mr. Lynch has no background in genetics, actively studies nothing (performs no research or clinical trials), and isn’t even a real doctor. But he’s the leading “expert” on MTHFR mutations and blames it for most problems we deal with – from heart disease to gut disorders.
Are we so desperate for help that we’ll turn to anyone who claims to be an expert? You don’t have to be. We’ve got your back!
What Lynch IS doing is simple. He’s reaching for fame and fortune by creating a new niche. He’s the guy that made the system that others can use to make revenue. He sells training to other “practitioners” telling them how they can leverage it to make themselves rich.
All they have to do is pay a kickback up the ladder and recruit people to the system and they get a piece of that. Wait a minute? Doesn’t that sound like something else we’ve discussed? It’s almost like it would take a shape if we drew it out:
Forbes did a great article on him and the “practice” in 2016 where I found this telling paragraph:
“He [Lynch] claims to teach how to create a million-dollar online business, as he allegedly did for himself while ‘in medical school.’ And through a pyramid-like incentive scheme, Lynch gives commission to SHEI members who recruit others into buying StrateGene and SHEI products.”
Emphasis mine. He’s not leading with “we can help your patients” but instead “you can get rich.”
At best, Lynch is taking a very liberal view of the data. What’s more realistic is that he is cherry picking out the small studies that show loose links between MTHFR/homocysteine and diseases while ignoring the data that contradicts these points. He’s trying to become rich using a gimmick that science shows is snake oil.
To be clear, MTFHR mutation isn’t one of those situations where the science is “incomplete.”
It’s not the promised land of understanding our bodies better than we ever had. It’s not the “undiscovered country” in medicine. It’s bad science. It’s the upside-down.
Don’t take him or anyone who promotes this seriously.
Homocysteine IS A Problem
When we first broached this topic in our 7 Deadly Deceptions rant, we made it very clear that we are empathetic to the people who do suffer from problems with their homocysteine methylation.
Some people DO have elevated homocysteine levels, and that can DEFINITELY be a problem. This is something we want to rectify if it is an issue.
We start first by saying, again, that you don’t need a genetic test here. Determining if you have a problem with homocysteine and MTHFR is cheap and easy. Treating it is even simpler.
In fact, most of us can prevent homocysteine issues by consuming enough protein and foods rich in B-Vitamins.
Food Sources of B Vitamins
- Fruits and vegetables, especially dark leafy greens, cantaloupe, beets, and oranges
- Whole grains
- Beans
- Eggs, poultry, fish, and organ meats
- Mushrooms
Gut bacteria play a role in making and consuming folic acid, so some people state it’s important to have a healthy gut to keep homocysteine in check.
I think that’s a stretch, but probiotics are a Vital 5 supplement for many reasons. It definitely won’t hurt to keep your gut bacteria as healthy as possible.
If we are deficient in one or more B Vitamins, using individual B-Vitamins or a B-Complex may help. Let’s start with the easy ones, then talk a bit about folic acid:
Vitamin B6
Vitamin B6 isn’t a single thing, but a group of vitamins that serve as a co-factor to about 100 different reactions in the body. It is often seen in supplements as pyridoxine, but we recommend people use the activated form of P5P (pyridoxine 5’-phosphate).
B6 is found in pork, turkey, bananas, chickpeas, potatoes, and dark chocolate. Even Dark Chocolate M&Ms!
Most of us have plenty of this from our diets, but many of our multivitamins and the like will have adequate B6 amounts.
Vitamin B12
B12 is another family of similar compounds that aid in numerous reactions in the body, specifically the manufacture of red blood cells.
There are three major types of B12: cyanocobalamin, hydroxocobalamin, and methylcobalamin. Methylcobalamin is the more active form of the three and is similar to activity and absorption to what we’d find in foods.
Many vegetarians or vegans may require B12 supplementation as B12 is found predominantly in animal products.
We recommend sublingual methylcobalamin as the GI tract has poor absorption, especially for people on acid-blocking drugs called PPIs.
Some people may require injections of B12 to get their numbers up as even sublingual absorption isn’t enough for some.
Vitamin B9 – Folic Acid
There is some confusion in the way Vitamin B9 is named. The term folates represents all folic acid compounds, in all their different forms. Folic acid is a common form found in vitamins and fortified foods, while foods naturally containing folate have a form called tetrahydrofolate (THF). There is a structural difference, which I believe is important.:
There is a difference between folic acid from foods vs their supplement counterpart, and it favors the supplement. Folic acid supplements taken with food are absorbed BETTER than from foods (85% vs 50%). It is also difficult to extract and stabilize the folates from food; most folic acid supplements will be synthetic in some way.
Ingested folic acid is converted to THF to l-methylfolate, which is used in the homocysteine/methionine loopty loop we talked about.
Long story short: we’ve never been a fan of using plain folic acid supplementation. We always prefer the more utilized, absorbable forms of the nutrients we supplement with. L-methylfolate or bust is our recommendation.
How much you should use is always up for debate by many, but it’s pretty set in stone by the NIH. Here’s the recommendation for intake of folic acid:
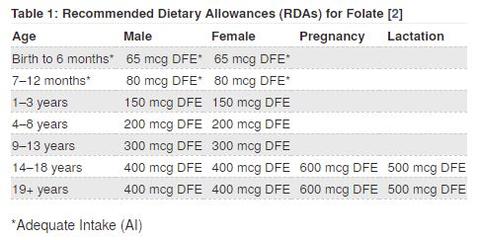
You’ll notice, of course, these numbers aren’t 1000-2000 mcg or more. They are low, compared to our perception of how much we need. The NIH also reports that most of us are doing fine by diet alone, but the numbers aren’t great for women of childbearing age, where folic acid deficiency is a problem.
High-dose l-methylfolate has been shown to be beneficial to some patients managing depression. That is a topic for another time!
Too Much Of A Good Thing
If you had elevated homocysteine levels, addressing the nutritional deficits or direct causes of elevated homocysteine is your best bet.
You can certainly address elevated homocysteine by utilizing B-Vitamins if they are shown to be deficient. They USUALLY are, so this is a safe bet. This is part of the mentality of a daily B-Complex; it’s better to be safe than sorry.
The quacks are mega-dosing people with methylated B-Vitamins to micromanage homocysteine levels that are usually not abnormal to begin with. The thing that has been shown time and time again is that mega-dosing supplements can have a U shaped effect:
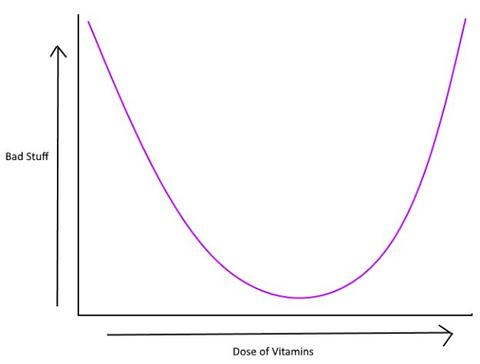
Basically, using supplements like B-Vitamins have a sweet spot where it helps, but overdoing it causes the same, if not more problems than the beginning. We call it a “U” shape because “U are getting hosed” by taking too many vitamins.
This brings me to my final rant point.I heard this, had an angry spell, read about it online, then had a mini-stroke… so you know it’s juicy!
Someone was instructed to megadose B-Vitamins to manage their homocysteine. On a follow up blood test, their numbers were EXCESSIVE. Way too high. What would you tell your patient? You’re right! Lower the dose, if not stop the supplement completely. That didn’t happen.
They were told by their “practitioner” that this was a sign that their body wasn’t utilizing B-Vitamins.
As if all of the trillion or so cells built a border wall to stop the caravan of B-Vitamins from entering. Except of course the cells of the GI tract and blood vessels that allowed the B-Vitamins to get there, those were working just fine.
I have a holiday analogy since it’s getting close: Does this mysterious condition turn the cells into all of the inns that rejected Mary and Joseph on Christmas Eve?
It’s absurd to state that high blood levels of B-Vitamins means that your body isn’t utilizing them. If your body wasn’t utilizing B-Vitamins, you’d be in BAD shape.
High B-Vitamins in your blood means exactly that: you’re being overdosed and have too much. Run away quickly from those who use this rationale.
My Good MTHFR’ing Recommendations
- Don’t get a genetic test for MTHFR mutations. Ever.
- If you have and you have a mutation, ignore it.You are not a mutant.
- If you would like, ask your doctor for a homocysteine, folic acid, and B12 level next time you get your bloodwork. It’s largely unnecessary.
- Supplement with low dose B12 and folic acid or other B’s in their more bioavailable forms, when necessary
- MethylB12 – 1,000mcg dissolved under the tongue
- L-Methylfolate – 400mcg for most of us, 1000mcg if you need a bit extra
- Coenzyme B Complex – 1 capsule daily
- If you DO have high homocysteine that you’d like to manage, we’ve got just the thing:
- Homocysteine Support – it has higher doses of folate and B12
You Look Good In Those Genes
I pulled this quote directly from one of the dopes’ websites:
“An increasing number of people have trouble metabolizing folate due to a genetic mutation of the MTHFR gene, which interferes with the production of the MTHFR enzyme. When that enzyme is dysfunctional, folate is not absorbed or utilized properly.”
There is no increasing number of people with difficulty metabolizing folate. There’s a new way to test to see if you have a problem that doesn’t exist.
While the rest of what they say is true: a genetic abnormality IS a real issue and problems with folate (either too little being absorbed or the inability to metabolize it) can be a HUGE problem. We should be active in monitoring for it and replacing missing nutrients vigilantly.
The big takeaway here is that we always have been vigilant. The diagnosis and treatment are cheap and easy. The complicated nature of this is created out of a desire to sell books, supplements, and a mindset.
MTHFR genetic mutations are not a problem that needs to be addressed UNLESS there actually is a problem, usually picked up on during annual physicals.
Taking megadoses of overpriced supplements WILL be harmful. And it’s all for naught, as there is no direct connection to elevated homocysteine and any of the diseases they say, besides cardiovascular disease.
If you love supplements and holistic wellness like we do, we should demand more integrity from the players. Don’t lend these so-called “experts” any credibility. Genetics isn’t everything here, in fact, it’s mostly nothing.
Just trying to keep it real…

Neal Smoller, PharmD
Owner, Pharmacist, Big Mouth
